 Spina bifida is a birth defect that involves the incomplete development of the spinal cord or its coverings. The term spina bifida comes from Latin and literally means "split" or "open" spine.
Spina bifida is a birth defect that involves the incomplete development of the spinal cord or its coverings. The term spina bifida comes from Latin and literally means "split" or "open" spine. Spina bifida occurs at the end of the first month of pregnancy when the two sides of the embryo's spine fail to join together, leaving an open area. In some cases, the spinal cord or other membranes may push through this opening in the back. The condition usually is detected before a baby is born and treated right away.
Types of Spina Bifida
The causes of spina bifida are largely unknown. Some evidence suggests that genes may play a role, but in most cases there is no familial connection. A high fever during pregnancy may increase a woman's chances of having a baby with spina bifida. Women with epilepsy who have taken the drug valproic acid to control seizures may have an increased risk of having a baby with spina bifida.
The two forms of spina bifida are spina bifida occulta and spina bifida manifesta.
Spina bifida occulta is the mildest form of spina bifida (occulta means hidden). Most children with this type of defect never have any health problems, and the spinal cord is often unaffected.
Spina bifida manifesta includes two types of spina bifida:
- Meningocele involves the meninges, the membranes responsible for covering and protecting the brain and spinal cord. If the meninges push through the hole in the vertebrae (the small, ring-like bones that make up the spinal column), the sac is called a meningocele.
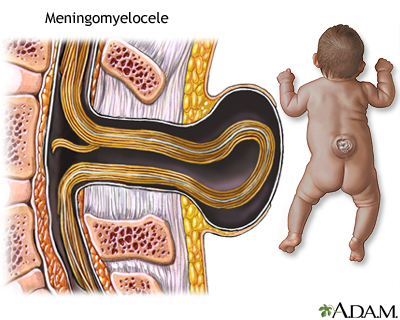
- Myelomeningocele is the most severe form of spina bifida. It occurs when the meninges push through the hole in the back, and the spinal cord also pushes though. Most babies who are born with this type of spina bifida also have hydrocephalus, an accumulation of fluid in and around the brain.
Because of the abnormal development of and damage to the spinal cord, a child with myelomeningocele typically has some paralysis. The degree of paralysis largely depends on where the opening occurs in the spine. The higher the opening is on the back, the more severe the paralysis tends to be.
Children with spina bifida often have problems with bowel and bladder control, and some may have attention deficit hyperactivity disorder (ADHD) or other learning difficulties, such as hand-eye coordination problems.
Diagnosing Spina Bifida
Expectant parents may be able to find out if a baby has spina bifida by taking certain kinds of prenatal tests.
The alpha-fetoprotein (AFP) test, performed between the 16th and 18th weeks of pregnancy, measures how much AFP, which the fetus produces, has passed in the mother's bloodstream. If the amount is high, the test is repeated because in many cases, high AFP readings are false. If the second result is high, other tests will be done to double-check and confirm the diagnosis.
Doctors also may use ultrasound to see if a baby has spina bifida; in some cases, the spinal defect can be seen on the ultrasound study. Amniocentesis also can help determine whether a baby has spina bifida. A needle is inserted through the mother's belly and into the uterus to collect fluid that is tested for AFP.
Maternal folic acid deficiency has been linked to spina bifida, and researchers believe that many cases can be prevented if women of childbearing age consume 0.4 milligrams (400 micrograms) of folic acid every day, and continue to take it throughout the first trimester.
It is important that folic acid consumption start before the onset of pregnancy to provide the best protection. Good sources of folic acid include eggs, orange juice, and dark green leafy vegetables. Many multivitamins contain the recommended dose of folic acid, too.
Symptoms of Spina Bifida
Babies who are born with spina bifida occulta often have no outward signs or symptoms. The spinal cord does not protrude through the skin, although a patch of hair, a birthmark, or a dimple may be present on the skin over the lower spine.
But other forms of the disease have obvious signs. Babies who are born with the meningocele form have a fluid-filled sac visible on the back. The sac is often covered by a thin layer of skin and can be as small as a grape or as large as a grapefruit.
Babies with myelomeningocele also have a sac-like mass that bulges from the back, but a layer of skin may not always cover it. In some cases, the nerves of the spinal cord may be exposed. A baby who also has hydrocephalus will have an enlarged head, the result of excess fluid and pressure inside the skull.
Treatment of Spina Bifida
Children with spina bifida occulta seldom need treatment.
In cases of spina bifida manifesta, treatment depends on the type of spina bifida and its severity.
Babies with meningocele usually have an operation during infancy in which doctors push the meninges back and close the hole in the vertebrae. Many will have no other health problems later unless there is nerve tissue involved with the sac.
Babies with myelomeningocele need more immediate attention and often have surgery within the first 1 to 2 days after birth. During this first surgery, doctors push the spine back into the vertebrae and close the hole to prevent infection and protect the spine.
A baby who also has hydrocephalus will need an operation to place a shunt in the brain. The shunt is a thin tube that helps to relieve pressure on the brain by draining and diverting extra fluid.
In addition, some children need subsequent surgeries to manage problems with their feet, hips, or spine.
The location of the gap in the back often dictates what kind of adaptive aids or equipment a child with myelomeningocele will need. Those with a gap high on the spinal column and more extensive paralysis often need to use a wheelchair, while those with a gap lower on the back may be able to use crutches, leg braces, or walkers.
Caring for a Child With Spina Bifida
Parents of children with spina bifida receive support from a medical team that may include several doctors (such as neurosurgeons, urologists, orthopedic surgeons, rehabilitation specialists, and general pediatricians), a nurse practitioner, physical and occupational therapists, and a social worker.
The goal is to create a lifestyle for the child and family in which the disability interferes as little as possible with normal everyday activities.